Best Practices for the Seldinger Technique
The Seldinger technique, also known as the Seldinger wire technique, is a medical procedure used to obtain safe access to blood vessels and other hollow organs. The procedure was introduced by Dr. Sven Ivar Seldinger in 1953 and was originally designed as a technique to improve aortography (examining the aorta).
The technique is used in a variety of clinical settings including Interventional Cardiology, Radiology and for insertion of central venous catheters. The Seldinger technique can also be used for suprapubic catheterisation.
About Suprapubic Catheterisation
A Foley catheter is required when a patient is unable to empty their bladder voluntarily. Suprapubic catheterisation requires the catheter to be inserted directly into the bladder via the abdominal wall. It is used for patients when urethral access to the bladder is not possible and/or desired.
Suprapubic catheters provide many benefits over urethral Foley catheters, including the reduction of CAUTI (Catheter Associated Urinary Tract Infection). You can find out more about suprapubic catheters in our page on the
Different Types of Catheters.
Suprapubic Catheterisation Using The Seldinger Technique
Without the Seldinger technique, healthcare professionals enter the bladder blind. The trocar is inserted directly through the abdominal wall forming a tract for catheter placement. This can lead to the perforation of the posterior of the bladder wall, as well as bowel damage.
A 2003 survey of British Urologists found that one third of respondents had experienced catheter associated bowel perforation in the previous 10 years[1]. A similar study, saw that 157 neuropathic bladder patients who were catheterised suprapubically without the Seldinger technique saw a 10% complication rate[2].
The Seldinger technique provides healthcare professionals with the alternative technique of suprapubic catheterisation which provides greater accuracy and control.
Steps to Perform Suprapubic Catheterisation Using The Seldinger Technique
1. Anaesthetic is injected to the entry site
2. A 1cm incision is made using a scalpel
3. A syringe is attached to the end of an 18-gauge needle and then inserted perpendicularly through the centre of the incision, using aspiration to locate the bladder
4. Following urine splash back, the syringe is removed from the needle
5. A guidewire is inserted through the needle, floppy end first. As it comes into contact and curves along the posterior wall of the bladder, the clinician will feel resistance and be able to stop the guidewire from being inserted too far which can cause damage to the bladder.
6. The needle is removed over the guidewire.
7. The sheath dilator is inserted into the bladder along the guidewire.
8. The dilator is removed from the outer sheath.
9. A Foley catheter is inserted down the sheath to the midpoint of the catheter length.
10. The balloon is inflated with 10ml of sterile water
11. The outer sheath slides back along the catheter shaft until it is external to the abdomen, at which point the sheath can be pulled apart and removed from the catheter.
Mediplus S-Cath™ System
Mediplus S-Cath™ System is designed to make suprapubic catheterisation safer, more efficient and easier for the healthcare providers. The guidewire has two black lines which help to guide the user into the bladder. Line 1 is used for inserting the needle and line 2 informs the healthcare provider when to stop inserting the sheath dilator.
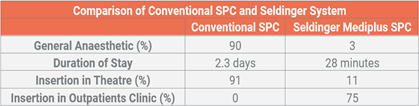
Increasing Theatre Capacity[3]
By inserting suprapubic catheters in an outpatient setting, theatre capacity demand is reduced. A study that compared a hospital’s clinical data over 2 years found large improvements with the Mediplus S-Cath™ System vs conventional suprapubic catheterisation. The results found:
Freeing up Consultant Time
Conventional suprapubic catheterisation without the Seldinger technique often requires consultants to either perform or be present during the procedure. In a study with 207 cases, 61.6% were performed in the presence of a consultant urologist[4].
Non-consultant grade clinical staff and nurse practitioners are able to perform the procedure after suitable training. This can free up time for consultants and enhance out of hours services.
Minimal Impact
The Mediplus S-Cath™ System grants clinicians a greater degree of control, allowing them to feel more confident when inserting the trocar into the bladder as access is maintained. This, combined with a reduction in the pressure needed to insert the trocar, results in reduced trauma and tissue damage for the patient.
If you would like to find out more about Mediplus S-Cath™ System, please visit our
product page.